GLP-1, GIP, and Glucagon: How Receptor Profile Shapes Research Outcomes
Single-pathway, dual, and triple agonists produce categorically different downstream effects. The receptor profile a molecule activates is the most consequential decision in any modern incretin-mimetic protocol.

The most important variable in modern incretin-mimetic research is rarely the molecule. It is the receptor profile the molecule activates. GLP-1 alone, GLP-1 plus GIP, and GLP-1 plus GIP plus glucagon are not three strengths of one idea. They are three different research instruments, each with its own downstream signature.
So choosing between Semaglutide, Tirzepatide, and Retatrutide is not a potency decision. It is a question of which mechanism you are trying to study. Get the receptor profile wrong for the question and the cleanest possible execution still produces the wrong data.
The incretin system, briefly
Incretins are gut hormones released after eating that prime the pancreas to respond to the meal. GLP-1 and GIP are the two principal ones. A 2019 review in Molecular Metabolism sets out GLP-1's core actions: glucose-dependent insulin secretion, appetite suppression, and slowed gastric emptying. The 'glucose-dependent' part matters, because it means the insulin response scales with glucose rather than firing regardless.
GIP is the second incretin, and historically the overlooked one. It influences insulin secretion and adipose-tissue signaling, and for years the assumption was that engaging it added little. The dual and triple agonists are partly a rejection of that assumption: they treat GIP as an arm worth pulling. Glucagon sits on the other side of glucose control, since it is the hormone that raises blood glucose, which makes its inclusion in a metabolic agonist look counterintuitive until you see how the receptor balance is engineered. GLP-1R, GIPR, and the glucagon receptor are the three building blocks the single, dual, and triple agonists draw from.
Single-pathway: Semaglutide as the reference
Semaglutide is the most-cited GLP-1 receptor agonist in metabolic research, and its value is its narrow specificity. It activates GLP-1R and recruits nothing adjacent. That makes it the natural control compound: when a study needs a known single-pathway reference to measure a dual or triple agonist against, semaglutide has the deepest literature behind it.
If a protocol needs a clean baseline for the glycemic and satiety pathways, this is the molecule. Everything more complex is, in effect, measured as a delta against it.
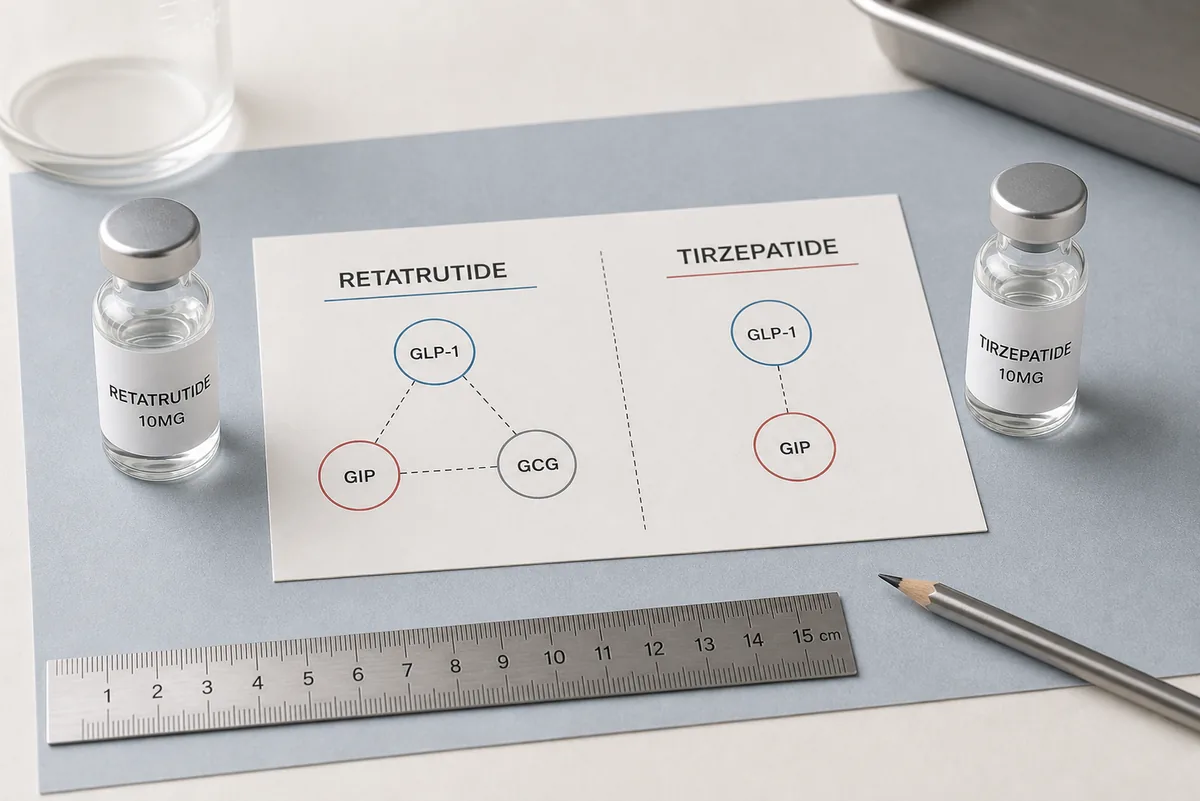
Dual agonism: the Tirzepatide signature
Tirzepatide adds GIP-receptor activation to the GLP-1 baseline. The 2018 Molecular Metabolism paper that introduced it characterized it as a single peptide engaging both receptors, and reported larger reductions in glucose and body weight in research models than selective GLP-1 agonism alone. The GIP arm amplifies the satiety signal and steepens the glycemic-response curve without amplifying GI-pathway side-effect signaling in the same proportion.
This is the receptor profile most current metabolic protocols treat as the dual-agonist standard. Where a single-pathway compound isolates one mechanism, Tirzepatide is the cleanest tool for studying how two incretin pathways interact, a question that did not have a clean instrument before dual agonists existed.
Triple agonism: Retatrutide and the glucagon axis
Retatrutide adds glucagon-receptor (GCGR) activation on top of GLP-1 and GIP. The 2022 Cell Metabolism paper that introduced it reported that, in obese-mouse models, the glucagon arm drove increased energy expenditure while the GIP and GLP-1 arms reduced caloric intake. The glucagon axis pulls hepatic energy metabolism and lipolysis into the response.
On its own, glucagon-receptor agonism would raise glucose. The triple agonist works because the receptor balance is tuned so the GLP-1 and GIP arms hold glucose handling steady while the glucagon arm adds energy expenditure. It is currently the most active investigational profile in the published metabolic literature, and studies on hepatic glucose output, lipid handling, or energy-expenditure modeling reference it as the canonical triple-agonist tool.
Why more receptors is not the same as more potent
A persistent misreading is that the triple agonist is just a stronger version of the single agonist. It is not. Each receptor arm recruits a different downstream system, so adding an arm changes the shape of the response, not only its size. A triple agonist studied as if it were a high-dose GLP-1 agonist will produce results that look like noise, because the glucagon and GIP contributions are not on the GLP-1 axis at all. The number of receptors is a qualitative variable wearing a quantitative disguise.
Choosing the right profile
The decision is not which is strongest. It is which receptor profile matches the hypothesis. A protocol built around glycemic-response kinetics is best served by single-pathway GLP-1. A protocol built around appetite-pathway interaction benefits from the dual agonist. A protocol built around hepatic energy expenditure is the canonical use case for the triple agonist.
Mismatching the compound to the question produces noise, not signal. The receptor profile is the experimental variable, and the molecule is just how that variable is delivered. The cleanest way to read what each additional receptor arm contributes is to run the single, dual, and triple agonists side by side and let the deltas between them do the talking.
For that comparative work, the practical risk is not the compounds but the lots. Sequence and purity have to be verified per-lot by independent HPLC and mass-spec analysis, and lots used in a single comparison should come from matched synthesis windows. Otherwise a difference that looks like a receptor effect can really be a lot-quality artifact, the kind of confound that quietly invalidates an otherwise clean design.
This article describes mechanisms and applications studied in research models. NZM peptides are sold strictly for in vitro and animal research. They are not for human consumption, off-label use, or clinical application.
From the desk.
Retatrutide vs Tirzepatide: Triple-Agonist vs Dual-Agonist Mechanism
Both are incretin-mimetic research peptides, but they engage categorically different receptor combinations. The mechanism distinction is what determines which one suits a given protocol.
Wegovy vs Ozempic: Same Compound, Different Brand Identity
Wegovy and Ozempic share the same active molecule (semaglutide). They are distinct branded products with different indications and dose strengths, but the mechanism is identical.
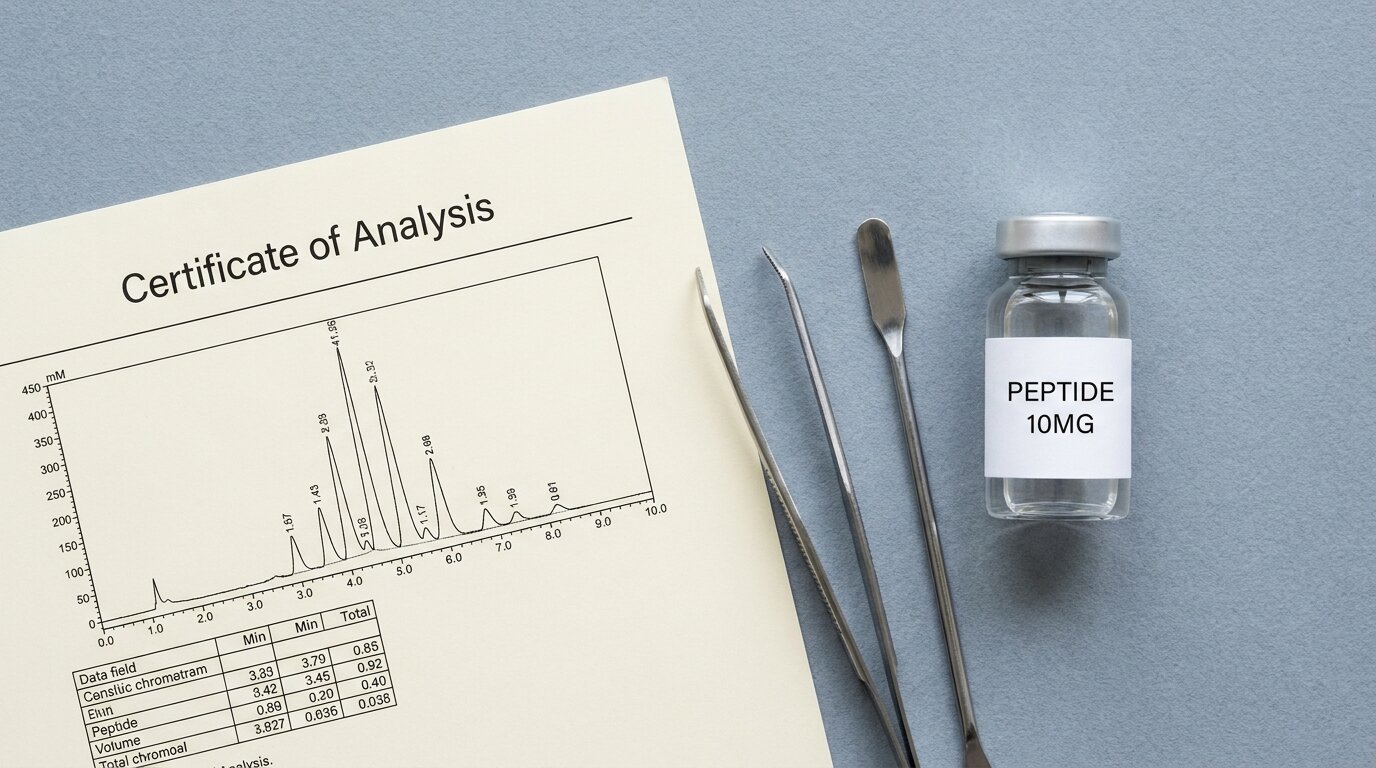
Why Janoshik Analytical: A Researcher's Guide to Independent Lab Verification
Independent third-party verification is the only credible way to certify what's actually in a research-grade peptide vial. Here's why Janoshik is the European reference, and what their COA actually tells you.